
Baseball is a popular summer sport that people of all ages watch and play. Although baseball is a limited-contact sport, there are common baseball injuries that occur due to the high velocity and repetitive nature of throwing. Whether you play pick-up baseball on the weekends with friends or participate in a league, you could be at risk of one of these injuries.
In this blog, we will explore the most common baseball injuries, how they occur, how to prevent them and how to get back to throwing safely.
Table of Contents
- Shoulder anatomy
- Common causes of baseball injuries
- Common baseball injuries
- Return to throwing protocol
- Conclusion
Shoulder Anatomy
Your shoulder is made up of the clavicle (collarbone), the scapula (shoulder blade) and the humerus (the upper part of the arm bone). The point where the scapula and humerus meet form the glenohumeral joint (the shoulder joint).
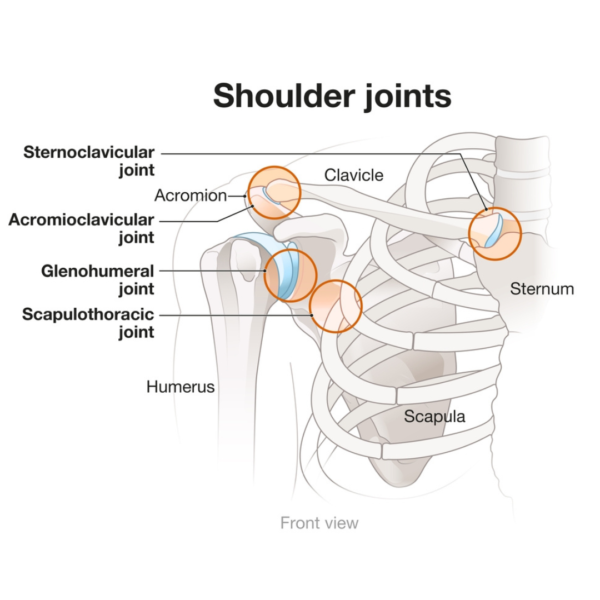
Think of the shoulder like a ball and socket. The scapula has a very narrow spot for the large humeral head to sit in. This is what gives our shoulder the large range of movement.
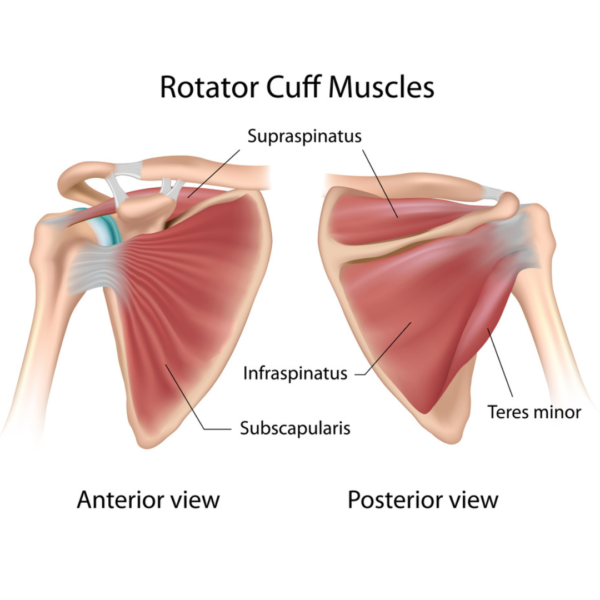
There are four muscles, collectively known as the rotator cuff, that help hold this joint altogether. The supraspinatus, infraspinatus, teres minor and subscapularis. These muscles make sure the humerus is held in place and provide it with the stability, but also help to move the arm in different directions.
Common Causes of Baseball Injuries
Injuries are common in baseball players due to the repetitive and high intensity throwing motions involved in the sport. Some reasons why injuries occur in baseball include:
Overuse: Many players throw the ball repetitively with significant force during games and practices. This puts constant strain on the shoulder joint and muscles and could lead to injury.
Throwing mechanics: If throwing mechanics are not properly aligned (such as an improper arm position) it can place excessive strain on the shoulder. With improper positioning the tendons are not in proper alignment and can cause increased stress on these structures and lead to injury.
Muscle imbalances: Insufficient strength of the shoulder muscles, and those surrounding the shoulder can also contribute to injury. It may result in the shoulder joint not having optimal stabilization and places the player at a higher risk of injury.
Common Baseball Injuries
Rotator cuff injuries:
There are four muscles, collectively known as the “Rotator Cuff”, that help hold the shoulder joint altogether. The supraspinatus, infraspinatus, teres minor and subscapularis. These muscles make sure the humerus is held in place and provide it with the stability, but also helps move the arm in different directions.
Presentation:
Rotator cuff injuries are common in baseball players, especially pitchers, due to the repetitive throwing motion. This motion puts excess stress on the rotator cuff tendons leading to injury, this can be an acute inflammation or a complete tear.
Players often present with pain in the shoulder area with possible radiating pain coming down the arm to the elbow. Pain may occur at rest, but it often gets worse with certain movements such as reaching, lifting, and throwing. Players with a rotator cuff injury might also present with limited range of motion in the shoulder and weakness which impacts their throwing velocity and accuracy.
Elbow Injuries
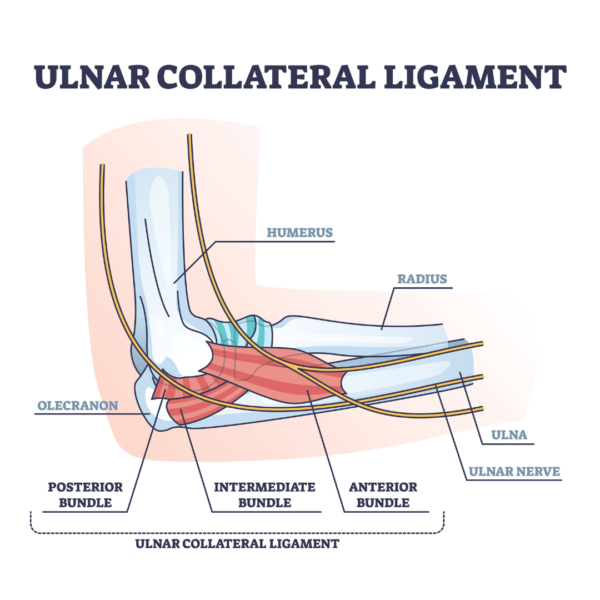
Our elbow is made of various ligaments that help hold the humerus (upper arm) and the ulna (our lower arm). The ulnar collateral ligament (UCL ligament) is a ligament that runs on the inside of the elbow that helps hold these to ligaments together and provides stability to the joint. In baseball, it is important for throwing motions.
Presentation:
Pitchers are prone to UCL injuries due to the repetitive high-velocity throwing motions. When the UCL has excessive stress placed on it, it can be come overstretched (leading to a sprain), partially torn to completely torn. Symptoms of a UCL sprain include pain on the inner side of the elbow joint, limited range of motion, possible tingling into the pinky and ring finger, weakness in gripping, and reduced throwing speed.
Return to Throwing Program
When rehabilitating a baseball player to return to throwing, it is important to consider that the type of injury and the degree of the injury (for example if it was an acute strain, long term overuse injury or a tear of a ligament or muscle) as it will impact the recovery time.
Position of the player must also be considered when returning to play as different positions require different demands on the arm. Return to throwing involves 4 main phases the player will progress through to prepare for play.[i]
Phase 1: Rest and Recovery
Initially the injured arm / elbow should be rested in order to heal. Sometimes, for elbow injuries, this might include a brace that limits the range of motion of the elbow to prevent more stretching of the UCL. During this phase your physiotherapist may use modalities such as ultrasound or laser to help reduce the inflammation. As the pain reduces, gentle range of motion will be introduced to help improve flexibility and reduce stiffness.
Phase 2: Mobility and Strength
This phase includes a progressive range of motion program to restore full elbow and/or shoulder mobility back to the player’s baseline. As range of motion improves, strengthening the muscles that surround the joint(s) is also important. This phase might also include strengthening muscles of the trunk and lower body. Strengthening exercises begin with low levels of strengthening such as exercises requiring submaximal contraction in midrange positions, and working up to strengthening at the end-ranges.
Phase 3: Throwing progression
At this stage, your physiotherapist will progress to asymptomatic plyometric strengthening and focusing on mechanics of throwing such as ensuring proper scapular positioning. Plyometric training involves powerful movements at high velocities which mimic the loads the player needs for play. Exercises will include with short-distance and low-intensity throws while focusing on proper form. Throwing distance will gradually increase while monitoring for any discomfort with the increase in intensity.
Phase 4: Return to full throwing
This stage will involve continuing to increase throwing distance, velocity and intensity. Sport-specific training will commence in this phase, specific to the patient’s position. During this stage the player will be working on returning to full game play and therefore a proper warm-up, cool-down and self-management strategies will be discussed by your physiotherapist in this stage to help reduce the risk of reinjury.
Prevention: It is important to note that injury prevention is also important with a sport like baseball. Below are a few considerations for prevention:
Warm-up: Players should participate in a dynamic warm-up before practices and games. This allows to increase blood flow to the muscles that will be used during play and improve flexibility.
Technique and Throwing mechanics: It is important for players to review their throwing, hitting and pitching mechanics, starting from a young age. Repetitive motion puts stress on the tendons/ligaments involved in the movement, however ensuring it is done correctly minimizes excess stress on the body and reduces the risk of overuse injuries.
Limit Pitch Counts: Recommended pitch counts will differ based on the player’s age. Rest periods in-between pitching and outings are also important to follow to avoid overuse injuries (like UCL sprains). In kids, this is crucial to follow to ensure healthy development of their arms. General pitch and rest recommendations based on the USA Baseball and American Sports Medical Institute are outlined below. However, some individuals may need more or less rest based on their conditioning, mechanics and developmental maturity.
Age 7-8:
- maximum of 50 pitches per game
- at least 1 day of rest after throwing
Age 9-10:
- maximum of 75 pitches per game
- at least 1 day of rest after throwing
Age 11-12
- maximum of 85 pitches per game
- at least 2 days of rest after throwing 66 or more pitches; at least 1 day of rest after throwing 36-65 pitches and no rest required for 35 or fewer pitches
Age 13-14
- maximum of 95 pitches per game
- at least 2 days of rest after throwing 76 or more pitches, at least 1 day of rest after throwing 26-75 pitches and no rest required for 25 or fewer pitches
It is also important to monitor the amount of throws over the course of the week (not just one day) to ensure there is proper rest provided and to prevent overuse injuries.
Strength and Conditioning: Age-appropriate strength and conditioning is important to be a part of the player’s routine to work on shoulder stability and strength.
Recognize signs of overuse and fatigue: Parents and coaches should recognize the importance of age-appropriate training and be aware of signs of overuse and fatigue to prevent injuries. Some signs to watch out for include:
- decreased performance (reduced accuracy, hitting power)
- complaints of pain in the shoulder or elbow after practices or games. Complaints of pain that lingers after a game or practice that does not improve with rest is also often an indication of an overuse injury.
- change in mechanics with throwing or hitting. This could be a sign the player is compensating due to fatigue or pain
- reduced endurance: decrease in the player’s endurance during practices o games is often a sign of tiredness
- changes in attitude: overuse and fatigue can lead to irritability or lack of enthusiasm for playing
- increased injury frequency: if the player is experiencing frequent minor injuries or recurring strains this is often a sign the body is unable to recover properly due to overuse
- change in shoulder range of motion indicate overuse-related stiffness or inflammation
Conclusion
Although there are various injuries that can occur with baseball, it is always important to talk to your physiotherapist on how to rehab and prevent the injuries from happening. Seeking the opinion of a healthcare practitioner early on helps with recovery to ensure you are provided with the proper rest and education needed to return to play.
Your physiotherapist can help ensure you return to play safely and reduce your risk of reinjury. Contact us at the clinic to ask how our therapists can help you!
Written by

OUR LOCATIONS
FOLLOW US!
OUR SERVICES










Last Updated on August 9, 2023 by Propel Physiotherapy





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}