
No two cases of diastasis recti are the same. As a result, diastasis recti physiotherapy or pelvic physiotherapy is based on an individual assessment by a trained professional. The results of this assessment will inform how we customize a treatment plan to address the symptoms connected to this condition.
There is an abundance of information on the internet and social media about diastasis recti. Unfortunately, the type of information found when scrolling or searching often leads to people feeling fearful and overwhelmed, and limiting their ability to seek help.
The truth is, when it comes to this condition, the research is significantly lacking and many of these fears are unfounded. This article aims to answer all of your burning questions and put to rest some of the strongly held myths about diastasis recti.
We will discuss the anatomical considerations of diastasis recti, the variety of treatment strategies, expectations for recovery and why an abdominal crunch might not be so bad after all. While diastasis recti may occur in children as well as men, this article will focus on diastasis recti during pregnancy and postpartum.
Table of Contents:
- What is diastasis recti?
- Possible symptoms connected to diastasis recti
- Possible symptoms connected to diastasis recti
- Myth 1: Diastasis recti means my abdominals are torn
- Myth 2: Diastasis recti is problematic
- Myth 3: Only certain individuals get diastasis recti during pregnancy
- Myth 4: Doing exercises like sit ups, crunches or planks will make my diastasis recti worse
- Myth 5: Surgery is the only option to “fix” diastasis recti
- Myth 6: “Coning and doming” are signs that I need to STOP doing an activity
- Myth 7: I’m not strong without my abs
- Possible symptoms connected to diastasis recti
- FAQ 1: Can diastasis recti be fixed with physiotherapy?
- FAQ 2: How do I know if I’m getting diastasis recti?
- FAQ 3: Should I see a physio for diastasis recti?
- FAQ 4: Will my diastasis recti ever go away?
- FAQ 5: How long does it take to heal diastasis recti with physical therapy?
- FAQ 6: What happens if diastasis recti goes untreated?
- FAQ 7: Does diastasis recti get worse with age?
- FAQ 8: What physio exercises are good for diastasis recti?
- FAQ 9: What exercises should you avoid with diastasis recti?
What is Diastasis Recti?
Diastasis recti, also knows as diastasis recti abdominis or DRA, refers to the midline separation of the abdominal muscles that is often associated with pregnancy but can also occur in children as well as men.
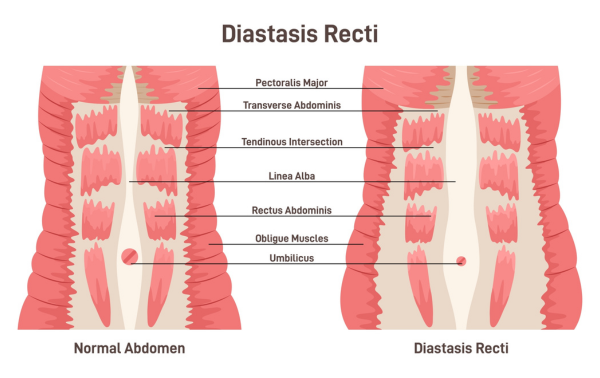
Diastasis recti refers to the stretching of the linea alba, or the widening of the gap between the two rectus abdomini muscles (what some refer to as the “six pack”). During pregnancy, the growing uterus exerts pressure on the linea alba (a fibrous band of connective tissue that runs vertically along the entire length of the abdominal wall). The linea alba responds to this pressure by increasing its width and thinning.
This is a completely normal adaptation that is necessary to accommodate a growing baby. In fact, studies have demonstrated that 100% of pregnant women have diastasis recti by gestational week 35. [i]
Possible Symptoms Connected to Diastasis Recti
As diastasis recti is a natural adaptation, there is no reason to expect problems or symptoms to accompany a DRA. In the postpartum period, the body experiences fluctuations and changes in everything from hormones to lifestyle, and there is a possibility that these adjustments result in physical symptoms. It’s important to not point the finger at one piece of the puzzle such as the abdominal wall, but to take a holistic approach when managing some of the following symptoms.
Possible symptoms connected to diastasis recti can include:
- Hip pain
- Low back pain
- Pelvic girdle pain
- Urinary or fecal incontinence
- Abdominal discomfort
- Symptoms of pelvic organ prolapse (bulging or heaviness felt at the perineum)
- Difficulty lifting heavy objects
*Important: These symptoms may be connected to diastasis recti, but diastasis recti is not necessarily the cause. If you are experiencing any of the above symptoms, check in with your pelvic health therapist for a thorough and holistic approach to treatment and recovery.
Biggest Myths About Diastasis Recti Busted
Myth 1: DRA means my abdominals are torn
Having diastasis recti does not mean anything is torn. As mentioned above, it refers to the widening of the space between the sides of the two rectus abdomini muscles. This space is often referred to as the “inter-rectus distance” (IRD). It is important to understand that the linea alba remains intact when we are talking about diastasis recti. Your abdominals are still connected! This is different than a hernia where tissues or organs can actually bulge through a weak point in the abdominal wall.
Myth 2: Diastasis recti is problematic
Many people who have diastasis recti abdominus do not experience pain. As tissues remain intact, there is often no physical discomfort associated with it. Misinformation has pathologized this common condition and expected result of pregnancy.
While some studies have found that diastasis recti may be associated with low back pain, other’s have found that it is not.[ii] Diastasis recti does mean there has been a change to the tissues of your abdominal wall. This has the potential to result in decreased core strength as well as altered body mechanics. Our core is a crucial component of support and stability, so it is possible that diastasis recti result in changes in our abilities to lift, run, jump or move how we used to before.
Keep in mind that our abdomen is not the only part of our core. The pelvic floor and our deep back muscles are also key components to the deep core system and should also be considered. Things to look out for which may require guidance from a health care professional include hip pain, low back pain, pelvic girdle pain, urinary or fecal incontinence, abdominal discomfort, symptoms of pelvic organ prolapse (bulging or heaviness felt at the perineum), or difficulty lifting heavy objects.
Myth 3: Only certain individuals get DRA during pregnancy
As mentioned, above, all pregnant people experience some form of diastasis recti during pregnancy. Our abdominal wall stretches and changes to accommodate the growing baby, just like other parts of the body adapt. Everyone has their own level of connective tissue stretching depending on factors like genetics, size of baby and body dimensions.
In the postpartum period, changes to the linea alba and abdominal wall vary greatly. Studies have shown that the prevalence of diastasis decreases to about 50% at 4-6 weeks postpartum and continues to decrease to 39% at 6 months postpartum.[iii]
For some individuals, the diastasis regresses to pre-pregnancy width shortly after pregnancy and functional strength is regained. For others, the extent of the separation is greater and despite interventions, resolution can require more time.
In some cases, the abdominal wall may never return to how it looked before pregnancy. In this case, it is important to remember that our bodies are meant to change with pregnancy. We should seek guidance and have expectations to return to function and fitness but encourage ourselves and each other that bodies may look different after bringing a human into this world.
Risk factors that have been reported for persistent diastasis recti include;
- Multiparity; multiple pregnancies
- Multiple gestation (twins, triplets, etc)
- Advanced maternal age[iv]
Myth 4: Doing exercises like sit ups, crunches or planks will make my DRA worse
Although sources may tell you otherwise, there is not sufficient evidence to support the notion that specific exercises such as sit ups, crunches or planks will make the separation worse. In fact, a recent study demonstrated that a 12-week program of abdominal curl-ups 5 days per week did not increase the separation but did result in improvements in abdominal muscle strength and fitness.[v]
If you are unsure if a movement of exercise is right for you, I highly encourage you to meet with a pelvic health physiotherapist for an individualized assessment. Chances are, you shouldn’t be avoiding anything you love or want to do!
Myth 5: Surgery is the only option to “fix” DRA
For the majority of the individuals with diastasis recti surgery is not required, but there are certainly situations when surgery becomes the best option. There is widespread agreement that physiotherapy should be the first line of treatment for diastasis recti. [vi]
Keep reading to learn more about the role physiotherapy can play in management of this condition. In some cases of advanced diastasis recti, surgical intervention is recommended, although it has been suggested that surgery should not be considered unless there is functional impairment or the presence of a hernia.[vii]
If surgery is recommended or desired, often the work you do with a physiotherapist beforehand and after is what will set you up for success. It’s important to remember that the linea alba tissue is an elastic connective tissue. Often there is a significant amount of natural resolution that occurs over the first year following childbirth. However, connective tissue heals slower than muscle, and for some individuals it may be worth taking a conservative approach for 18 months to two years before considering more invasive procedures such as surgery.
Myth 6: “Coning and doming” are signs that I need to STOP doing an activity
Outward “coning” or “doming” along the linea alba shows us that intra-abdominal pressure is increasing and pushing outwards on the softest wall of our deep core system.
Let’s consider two types of doming:
- “Soft Doming”: When you push on the linea alba, it feels soft and you can continue to push down and feel the edges of rectus abdominis
- “Hard Doming”: When you push on the linea alba, it feels hard and similar to the contracted rectus abdominis
If soft doming is occurring, there is still some “give” in the linea alba which means you are not pulling it tight to the end range. In this scenario, it is unlikely that the linea alba will stretch over time. If hard doming is occurring, then you are possibly taking the linea alba to its end range and therefore it could stretch more over time.
Doming is therefore something to be aware of, but not scared of. It can help to determine your threshold for load and activities. Hard doming should be avoided in repetition as it may lead to further stretching of the linea alba. [viii]
Myth 7: I’m not strong if I have diastasis recti
Many individuals who have diastasis recti are both strong and high functioning. Diastasis recti can occur (and persist) in elite athletes who have solid foundational strength. Most athletes can continue to do what they love with a diastasis.
The entire body changes with pregnancy and it’s very important to zoom out to look above, below and behind the abdomen. Our “core” consists of the deep abdominal muscles, the pelvic floor, respiratory diaphragm, and deep back muscles.
A pelvic health physiotherapist can complete a thorough assessment of the entire body to determine a treatment program that targets all the areas of the body that may contribute to your symptoms.
Most Frequently Asked Questions About Diastasis Recti
FAQ 1: Can diastasis recti be fixed with physiotherapy?
Diastasis recti physiotherapy provided by a registered physiotherapist trained in pelvic health can help in the following ways:
- Targeted strengthening: Studies have shown that deep core stability exercises can be effective in decreasing the inter-recti separation as well as improving postpartum women’s quality of life. [ix] [x] Strengthening programs should be individualized and progressive, using a variety of heavy loads. A trained physiotherapist can help you to find that “sweet spot” of challenging exercises that facilitates the natural process of healing.
- Posture and breathing: Small changes to the way the body stands, sits, moves and breathes can impact the way our deep core works, the way intra- abdominal pressure is managed and in turn may result in reduction of the separation.
- Assessment of the pelvic floor: Pelvic floor tension or weakness impacts the rest of the deep core and therefore can contribute to symptoms of diastasis rectus abdominus. A pelvic health physiotherapist may do an internal and/or external assessment of the pelvic floor and how it coordinates with the rest of your core system.
Activity modification: While there isn’t sufficient evidence to support the notion that certain activities will make diastasis recti worse, it can be extremely helpful to strategize on how to make a movement more efficient or less bothersome. Physiotherapists are movement specialists who have the ability to make minor changes to way you move in order to empower you to keep on moving.
FAQ 2: How do I know if I’m getting diastasis recti?
There may be no signs other than a change in the appearance of your abdominal wall. You may notice an outward “bulge” along the centre of the abdomen which is increased under load (ex: when going from lying to sitting, when carrying something heavy).
Other possible symptoms that are potentially connected to diastasis recti include difficulty lifting heavy objects, hip pain, low back pain, pelvic pain, urinary or fecal incontinence, symptoms of pelvic organ prolapse.
FAQ 3: Should I see a physio for diastasis recti?
Physiotherapists are movement experts and are positioned in a way to complete a holistic assessment of the signs or symptoms you are experiencing. If your diastasis recti is not bothersome, there may be no need to see a physiotherapist.
However, if you are experiencing any of the symptoms listed above, a physiotherapist trained in pelvic health and specifically DRA management is a great health professional to seek guidance from. Lastly, if you are not experiencing any symptoms, but are bothered by the look of your diastasis, that is also a completely valid reason to seek guidance from a physiotherapist.
FAQ 4: Will my diastasis recti ever go away?
“Recovery” from diastasis recti is difficult to predict. As mentioned above, targeted, progressive abdominal strengthening has been shown to have positive effects on diastasis recti including decreasing the inter-rectus distance (space between the two rectus abdomini muscles). Not everyone achieves full recovery with a conventional approach, but this is certainly the recommended first line of treatment prior to consideration of surgery.
FAQ 5: How long does it take to heal diastasis recti with physical therapy?
Each individual is different and the amount of time to “heal” or “recover” from diastasis recti will vary based on factors like the size of the separation, activity levels, lifestyle, hormone status, body dimensions, genetics and movement patterns. For many individuals, significant reduction of the “gap” occurs naturally within 4 to 6 weeks postpartum.[xi]
If your diastasis is taking longer to improve and you are working with a physiotherapist, keep in mind that connective tissue heals slower than muscle. It may therefore be worth waiting up to 18 months to see results. Ultimately this time should be spent progressively overloading the abdominal wall to promote tissue adaptations and structural change.
FAQ 6: What happens if diastasis recti goes untreated?
As mentioned above, diastasis recti is not necessarily problematic. Most people do not experience pain with diastasis recti alone. If you are experiencing functional limitations or would like to change the appearance of your abdominal wall, guidance from a physiotherapist is likely to help optimize your recovery and potentially speed along the natural closure of the gap.
FAQ 7: Does diastasis recti get worse with age?
Diastasis recti has the possibility of getting “worse” with factors that may be associated with aging such as decreased activity levels as well as weight gain. As we age, hormones and activity levels may change which have the possibility of impacting the abdominal wall, tissue strength and appearance. It is never “too late” to seek guidance on the best way to manage your diastasis recti.
FAQ 8: What physio exercises are good for diastasis recti?
There is no evidence to support that a single exercise will resolve diastasis recti. As mentioned above, there is evidence that core strengthening and stability exercises that are individualized, progressive and use a variety of heavy loads can be effective.
It is also important to ensure you are strengthening in multiple positions – not just on your back. Challenge the whole system by working within your tolerance in lying, side-lying, 4-point, sitting, standing. Your physiotherapist is a great resource for exercises that are progressive, functional and right for you.
FAQ 9: What exercises should you avoid with diastasis recti?
There isn’t sufficient evidence to support the notion that we should avoid specific exercise with diastasis recti. A better guide would be to draw awareness of soft and hard doming (see “Myth # 6). We want to ensure that we are not doing exercises that exceed the tolerance of our tissues, but at the same time, we need to challenge those tissues in order to develop strength and endurance.[xii]
More recent experts in the field are suggesting that we need to progressively overload the abdominal wall in order to get hypertrophy (growth) of muscles such as the rectus abdominis and therefore see structural changes.
Diastasis Recti Physiotherapy Conclusion
Diastasis recti abdominis can seem like a scary and overwhelming condition to manage. If you are postpartum and experiencing diastasis recti, please remind yourself that your body is meant to change to allow the gift of growing and delivering a baby. On the other hand, if your body is not functioning or looking the way you would like it to, evidence does support physiotherapy as a first line treatment or management option for this condition.
All women develop some degree of diastasis recti by the third trimester. Working with a pelvic health physiotherapist can certainly result in greater body awareness, improved strength and function of your deep core muscles, optimal body mechanics including posture and breathing, and enable you to return to activities you love.
These in turn, may very well result in structural changes of the abdominal wall and a “flatter” stomach. However, it should be emphasized that pregnancy is likely to result in changes in one’s tissues, including muscle, fascia and skin.
For some individuals, these changes cannot be reversed with diastasis recti physiotherapy or surgery. It’s time to reject the “bounce back” culture that places unrealistic expectations on child-bearing bodies. Let’s challenge the postpartum body for what it can do, not how it appears!
If you are experiencing symptoms connected to diastasis recti, contact us for a complimentary consultation and find out how a customized diastasis recti physiotherapy treatment plan can help.
References
[i] Mota PG, Pascoal AG, Carita AI, Bo K. Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartu, and relationship with lumbo-pelvic pain. Manual therapy. 2015 Feb 1; 20 (2): 200-5.
[ii] Gbolabo Sokunbi, Gaston Camino-Willhuber, Philip K. Paschal, Oluseun Olufade, Farah S. Hussain, Jennifer Shue, Celeste Abjornson, William D. Zelenty, Darren R. Lebl, Frank P. Cammisa, Federico P. Girardi, Alexander P. Hughes, Andrew A. Sama. Is Diastasis Recti Abdominis Associated With Low Back Pain? A Systematic Review. World Neurosurgery, Volume 174, 2023, Pages 119-125, ISSN 1878-8750, https://doi.org/10.1016/j.wneu.2023.03.014.
[iii] Mota PG, Pascoal AG, Carita AI, Bo K. Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Manual therapy. 2015 Feb 1; 20 (2): 200-5.
[iv] Candido G, Lo T, Janssen PA. Risk factors for diastasis of the recti abdominis . Journal of the Association of Chartered Physiotherapists in Women’s Health 2005; 97: 49–54.
[v] Sandra B Gluppe, Marie Elston Engh, Kari Bø. Curl-up exercises improve abdominal muscle strength without worsening inter-recti distance in women with diastasis recti abdominis postpartum: a randomised controlled trial.
Journal of Physiotherapy, Volume 69, Issue 3, 2023, Pages 160-167, ISSN 1836-9553, https://doi.org/10.1016/j.jphys.2023.05.017.v
[vi] Mommers EHH, Ponten JEH, Al Omar AK, et al.: The general surgeon’s perspective of rectus diastasis. Surg Endosc 2017;31(12):4934–4949.
[vii] Carlstedt A, Bringman S, Egberth M, Emanuelsson P, Olsson A, Petersson U, Pålstedt J, Sandblom G, Sjödahl R, Stark B, Strigård K, Tall J, Theodorsson E. Management of diastasis of the rectus abdominis muscles: recommendations for swedish national guidelines. Scand J Surg. 2021 Sep;110(3):452-459. doi: 10.1177/1457496920961000. Epub 2020 Sep 28. PMID: 32988320; PMCID: PMC8551433.
[viii] Lo, Antony. Diving into Diastasis. My PT Education. PDF Retrieved Online
[ix] Thabet AA, Alshehri MA. Efficacy of deep core stability exercise program in postpartum women with diastasis recti abdominis: a randomised controlled trial. J Musculoskelet Neuronal Interact. 2019 Mar 1;19(1):62-68. PMID: 30839304; PMCID: PMC6454249.
[x] Core strengthening: Benjamin DR, Van de Water ATM, Peiris CL. Effects of exercise on diastasis of the rectus abdominis muscle in the antenatal and postnatal periods: a systematic review. Physiotherapy. 2014;100(1):1-8. doi:10.1016/j.physio.2013.08.005
[xi] Mota PG, Pascoal AG, Carita AI, Bo K. Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Manual therapy. 2015 Feb 1; 20 (2): 200-5.
[xii] Antony Lo. (2023). Diastasis: Current Concepts for Affective Assessment and Management. [Webinar] My PT Education. RECORDING: Webinar – DIASTASIS: Current Concepts for Effective (teachable.com)
Written by

OUR LOCATIONS
FOLLOW US!
OUR SERVICES



Last Updated on July 23, 2024 by Propel Physiotherapy




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}