
A physiotherapist with experience in leg amputation rehabilitation can work with individuals after surgery to create an individualized treatment plan based on their physical status and rehabilitation goals. Learning to use a wheelchair and walk with prosthesis are part of larger functional goals that are often included in the rehabilitation treatment plan.
Each year, several thousand Canadians undergo leg amputation surgery as a result of diabetes, trauma, vascular disease, and for many other reasons. A multidisciplinary team of healthcare professionals will work with these individuals to manage their physical and mental health, relearn essential skills and adapt to tasks for work and daily living.
In this article, we discuss the different types of lower limb amputation, primary conditions leading to, and complications associated with amputation. We will also list the healthcare providers and their role in the treatment process before detailing the ways physiotherapy can help rehabilitation after a leg amputation.
Table of Contents:
- What is a leg amputation?
- Different types of lower limb amputations
- Causes of lower limb amputations in Canada
- Potential complications after a leg amputation
- Treatment after leg amputation
- Types of prosthesis
- Physiotherapy for leg amputation rehabilitation
- Conclusion
What is a leg amputation?
Amputation refers to the removal of a limb due to injury, disease, or surgery. The lower limb is the part of the body that includes the leg, knee, ankle and foot.
There are multiple causes associated with leg amputation, including complications of diabetes or vascular diseases, trauma, congenital limb deformities, and bone cancer.
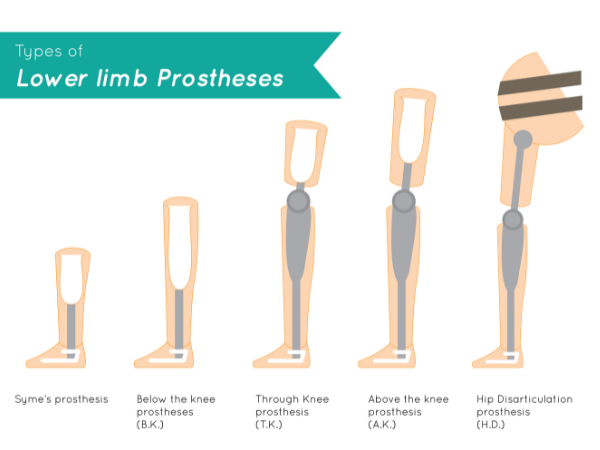
Different types of lower limb amputations
Amputations can happen at any point in the lower limb. Generally, the lower the amputation, the more joints that are spared, the better the potential for a more normal walking pattern with a prosthesis.
- Foot, including toes or partial foot
- At the ankle (ankle disarticulation)
- Below the knee (transtibial)
- At the knee (knee disarticulation)
- Above the knee (transfemoral)
- At the hip (hip disarticulation)
Causes of Lower Limb Amputations in Canada
The primary cause of leg amputations in North America is complications of diabetes, which account for 65% of all cases. The mean age at amputation is 65.7 (±16.6) years old and 68.8% of individuals who undergo an amputation are male.
Transtibial (lower leg) amputations are the most common compared to other levels. The average age-adjusted rate of leg amputation in Canada from April 1, 2006, to March 31, 2012, was 22.9 per 100 000. The lowest rates were in Quebec and British Columbia, and the highest rates were in Newfoundland and Labrador.[i]
Possible complications after a leg amputation
There are several complications related to amputation such as infection, phantom limb pain, residual limb pain, slow wound healing, vascular issues and necrosis, neuromas, edema, and skin breakdown.
Phantom pain is a common occurrence after an amputation and is perceived in the limb that has been removed from the body. It is typically characterized as a sharp or burning pain that occurs due to a miscommunication of nerve signals from the brain to the spinal cord.
Treatment After Leg Amputation
Treatment after a leg amputation is multidisciplinary and may involve the following professionals:
- Orthopaedic surgeon – surgical management and post operative follow up
- Physiatrist – pain management as well as management of complications that may arise
- Family doctor – general health monitoring and management of associated conditions, such as diabetes or peripheral vascular disease
- Prosthetist – fabrication and adjustments of a prosthesis
- Physiotherapist – gait training with a prosthesis, strengthening, normalization of joint range of motion and muscle length-tension, pain management
- Occupational therapist – equipment accommodations and job evaluation/re-training, as well as teaching individuals how to adapt to life without a prosthesis
- Social worker/counsellor – for emotional support and coping strategies, as well as providing access to community resources
Types of Prostheses
There are many different prosthesis options that are chosen according to an individual’s physical status, location of amputation, and functional goals.
Check out Prosthetic Leg Fit: Types of Knee Prosthesis for an overview of above knee amputations prosthetics.
Physiotherapy for Leg Amputation Rehabilitation
Physiotherapy after a lower limb amputation begins in the hospital during an individual’s acute care stay. Physiotherapists help teach new amputees how to use a wheelchair and other gait aids such as walkers and crutches, and how to complete different types of transfers.
Prior to being fitted with a prosthesis, individuals should work with a physiotherapist to strengthen the muscles of the residual limb and the sound limb, and to ensure range of motion of the remaining joints is within functional limits. The wound from the amputation and the swelling in the residual limb will need time to resolve prior to being fitted with a prosthesis.
Once individuals are fitted with a prosthesis, the physiotherapist will work in conjunction with the prosthetist to assess their standing posture, balance, and gait, and recommend any necessary adjustments. This is often a continual process throughout the rehabilitation continuum in acute care, inpatient rehabilitation, and outpatient community settings.
Physiotherapists will help individuals learn to walk with their new prosthesis, first in the parallel bars or with a walker, and then, depending on the individual, wean off gait aids and work toward walking independently.
There is a great deal of core strength, hip strength, as well as balance and coordination required to learn how to walk with a prosthesis and rehabilitation is often a lengthy process that continues after the individual has been discharged home.
Additionally, individuals who have undergone an amputation will often require multiple sockets as their residuum shrinks and may need different types of prostheses as they go through the rehabilitation process, all of which require some degree of retraining and adjustment.
The nature of rehabilitation after a leg amputation at or above the knee will depend on the client’s goals and physical presentation but will often include:
- Gait assessment and prosthesis training – analyzing the gait pattern for any compensations and deficiencies and providing facilitation techniques as well as a tailored exercise program to address these
- Collaboration with the prosthetist on adjustments to the prosthesis
- Wheelchair skills training – individuals with leg amputations will often require a wheelchair at least some of the time. Physiotherapists are trained to instruct individuals in the skills requires to navigate the community in a chair, including popping curbs, breaking down and setting up the chair for transportation, wheelies, ramps, and stairs.
- Gait aid training – teaching individuals to use walkers, crutches, and canes with or without their prosthesis.
- Transfer training – instruction of how to transfer to different types of surfaces including bed to chair and teaching individuals how to get on and off the floor
- Static and dynamic balance training – static balance training refers to training standing balance with a prosthesis, on different types of surfaces (foam pads, Bosu ball) and with eyes open and closed. Dynamic balance refers to the ability to maintain balance throughout motion, such as walking, running, crossover stepping, and stairs. Both balance components are very important when an individual is learning to use a prosthesis in a community setting.
- Strengthening the hip muscles of the residual limb, as well the muscles of the sound leg, and core – this is done through therapeutic exercise in clinic as well and a graded and progressive home exercise program that is completed independently.
- Desensitization techniques / mirror box therapy – used as a treatment technique for individuals experiencing phantom pain. Mirror therapy involves the individual blocking the view of their amputated leg with a mirror which is reflecting the view of the person’s sound leg. This gives the visual illusion that the individual has two sound legs which are moving together and can help lessen the individuals experience of phantom pain. Mirror therapy can be combined with desensitization techniques on the amputated limb, progressing from very soft textures on a non-painful point to rougher textures.
- Manual therapy – techniques used by physiotherapists to normalize muscle tension and joint mobility
- Edema management – compression therapy and soft tissue mobilization/lymphatic drainage to aid in the resolution of edema in the residuum
- Education on activity modification and return to recreational activities – physiotherapists work with each individual to establish their goals for return to functional activities, then create a unique treatment plan that is tailored to them.
Conclusions
When an individual has undergone a lower limb amputation, learning to use a prosthesis is often a crucial step in the rehabilitation process. A well-fitting prosthesis can help individuals regain mobility and return to their daily activities. This allows the freedom and independence to get back to doing the activities that are important to them.
The physiotherapists at Propel Physiotherapy are trained in the rehabilitation of individuals who have undergone an amputation. They will work with you to explore your individual needs and rehabilitation goals and create an individualized treatment plan. If you have any questions about amputation rehabilitation, please reach out to us at info@propelphysiotherapy.com or 416-621-2506 to schedule a complimentary consultation with one of our clinicians.
References
[i] Imam B, Miller WC, Finlayson HC, Eng JJ, Jarus T, Incidence of lower limb amputation in Canada. Can J Public Health 2017;108(4):e374–e380 doi: 10.17269/CJPH.108.6093
Written by






{kind=link}
{kind=link}