
Club foot is a common birth defect that affects muscles and bones in the feet. The condition does not resolve with growth and can lead to serious problems, including the inability to walk. Club foot treatment is essential to ensuring proper alignment and healthy development of the child.
Physiotherapy for club foot is an integral aspect of the comprehensive treatment approach aimed at correcting foot deformities and promoting optimal function. In this blog, we look at the various types of club foot, a three-step club foot treatment approach and the role of physiotherapy in managing club foot.
Table of Contents
- What is idiopathic club foot?
- Other types of club foot
- Club foot treatment
- Physiotherapy for club foot
- Conclusion
What is Idiopathic Club Foot?
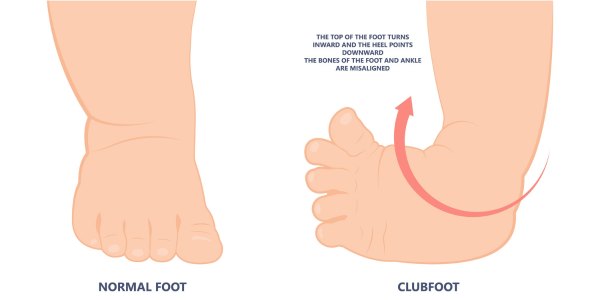
Club foot, also known as talipes equinovarus, manifests in various forms. Idiopathic club foot is the most prevalent. It presents at birth with the foot turned down and inwards due to a shortened Achilles tendon, affecting approximately 1 in 1000 babies.
This type often involves smaller and misaligned bones and tendons on the affected side. Half of all cases involve only one foot, with boys being twice as likely as girls to be affected. While the exact cause remains unclear, factors like familial history and maternal smoking during pregnancy may elevate risks. Diagnosis usually occurs via prenatal ultrasound and physical examination post-birth.[i]
Other Types of Club Foot
Other types of club foot expand beyond the idiopathic form and encompass neurogenic and syndromic varieties.
Neurogenic club foot arises from underlying neurological conditions such as cerebral palsy or spina bifida, leading to foot deformities that may manifest later in childhood rather than at birth. These conditions disrupt the normal function of nerves controlling muscle movement, resulting in abnormalities in foot positioning.[ii]
Syndromic club foot is associated with various syndromes characterized by multiple symptoms beyond foot deformities. Syndromes linked to club foot include arthrogryposis, which involves joint contractures, constriction band syndrome, tibial hemimelia featuring partial or complete absence of the tibia, and diastrophic dwarfism, marked by skeletal dysplasia and joint deformities. These syndromes often present complex challenges requiring multidisciplinary care approaches to address both foot abnormalities and associated systemic issues.[iii]
Club Foot Treatment
Treatment for talipes equinovarus, commonly known as club foot, is essential as the condition does not resolve spontaneously with growth. Treatment typically involved a 3-step process, including casting, surgical intervention and bracing, which is then typically followed by physical therapy.
Serial Casting
The Ponseti method, a widely adopted approach, involves serial casting to gradually correct foot deformities. This method commences within 1-2 weeks after birth, with casts changed every 7-10 days over a period typically requiring 4-9 casts. Casting aims to reposition the foot into a more neutral alignment, facilitating weight-bearing through the sole. [iv]
Club Foot Surgery
Casting alone may not fully address the downward foot position, necessitating surgical intervention, particularly an Achilles tendon release, to alleviate tension and achieve neutral alignment. In some cases, ligament surgery may also be required. Following surgery, a final cast is applied for approximately three weeks before initiating the bracing protocol.
Bracing
Bracing plays a crucial role post-casting and surgery to prevent club foot recurrence. Without bracing, there is a high risk of recurrence, approaching 100%, emphasizing its importance in maintaining correction.
Bracing involves utilizing a supramalleolar orthosis with a spacer bar, maintaining heels at shoulder width apart and feet outwardly rotated with toes slightly pointed up. Even if club foot affects only one side, bracing is applied bilaterally to ensure proper alignment.
Initially, children wear braces for 23 hours daily, removing them only for hygiene and exercises, gradually tapering down to 12 hours daily if regression isn’t observed. Additionally, children often wear braces during naps and nighttime until around 4-5 years old to consolidate correction and prevent relapse. This comprehensive treatment approach aims to achieve and sustain optimal foot alignment, promoting normal function and mobility throughout development.[v]

Physiotherapy for Club Foot
Physiotherapy intervention plays a pivotal role in the comprehensive management of club foot (talipes equinovarus), encompassing various therapeutic modalities aimed at optimizing foot function and promoting proper musculoskeletal development.
Stretching exercises are integral, involving both in-clinic sessions and home-based programs prescribed to parents to maintain foot flexibility.
Strengthening exercises target specific muscle groups, including those on the outside and front of the lower leg, as well as hip and knee muscles, crucial for maintaining proper foot alignment during functional activities. For older children, exercises such as squatting, standing on one foot, and frog jumps are employed to enhance muscle strength and coordination.
Gait training is emphasized to correct foot positioning before the child commences walking independently. This corrective approach ensures the promotion of efficient gait patterns and the correction of any deviations, facilitating optimal mobility.
Balance and proprioception training are implemented to enhance spatial awareness and stability, utilizing various surfaces like foam mats or Bosu balls to challenge the child’s balance and strengthen muscles around the foot and ankle, facilitating proper alignment during gait and functional tasks.
Functional retraining focuses on supporting the child’s ability to perform daily activities as they grow, including tasks like ascending and descending stairs, transitioning from sitting to standing, and engaging in recreational activities such as jumping or kicking a ball.
Physiotherapists provide education and monitoring, assessing skin integrity to prevent brace-related complications and collaborating with orthotists to address any brace-related issues.
Taping techniques may be utilized post-bracing to provide gentle positioning guidance for the foot, aiding in maintaining correction.
Moreover, physiotherapists employ various modalities such as heat, ice, soft tissue release, and ultrasound for pain relief, addressing any discomfort associated with the condition or therapeutic interventions.
Conclusion
Through a multifaceted approach encompassing stretching, strengthening, gait training, and functional retraining, physiotherapy aims to optimize outcomes and enhance the quality of life for individuals with club foot, ensuring proper musculoskeletal development and functional independence.
Ultimately, successful intervention aims to achieve optimal foot positioning and flexibility, enabling normal activity and function into adulthood. However, around 20% of treated children may require additional interventions later due to residual muscle imbalances. Through comprehensive treatment and ongoing support, individuals with club foot can lead active, unrestricted lives.
For more information about club foot treatment and physiotherapy, contact us to set up a complimentary 15-minute phone consultation.
Written by

OUR LOCATIONS
FOLLOW US!
OUR SERVICES



Last Updated on May 22, 2024 by Propel Physiotherapy





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}